Two drugs are better than one for ovarian cancer (Karen Ring). Earlier this week, scientists from UCLA reported that a combination drug therapy could be an effective treatment for 50% of aggressive ovarian cancers. The study was published in the journal Precision Oncology and was led by Dr. Sanaz Memarzadeh.
Women with high-grade ovarian tumors have an 85% chance of tumor recurrence after treatment with a common chemotherapy drug called carboplatin. The UCLA team found in a previous study that ovarian cancer stem cells are to blame because they are resistant to carboplatin. It’s because these stem cells have an abundance of proteins called cIAPs, which prevent cell death from chemotherapy.
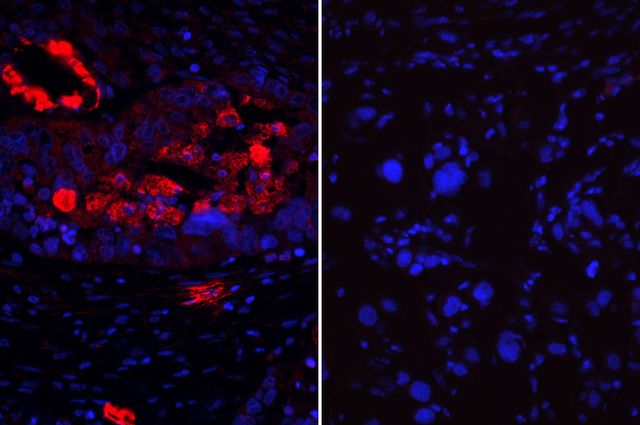
Ovarian cancer cells (blue) expressing cIAP protein (red) on the left are more sensitive to a combination therapy than cancer cells that don’t express the protein on the right. (UCLA Broad Stem Cell Research Center/Precision Oncology)
Memarzadeh discovered that an experimental drug called birinapant made some ovarian cancer tumors more sensitive to chemotherapy treatment by breaking down cIAPs. This gave her the idea that combining the two drugs, birinapant and carboplatin, might be a more effective strategy for treating aggressive ovarian tumors.
By treating with the two drugs simultaneously, the scientists improved the survival rate of mice with ovarian cancer. They also tested this combo drug treatment on 23 ovarian cancer cell lines derived from women with highly aggressive tumors. The treatment killed off half of the cell lines indicating that some forms of this cancer are resistant to the combination treatment.
When they measured the levels of cIAPs in the human ovarian cancer cell lines, they found that high levels of the proteins were associated with ovarian tumor cells that responded well to the combination treatment. This is exciting because it means that clinicians can analyze tumor biopsies for cIAP levels to determine whether certain ovarian tumors would respond well to combination therapy.
Memarzadeh shared her plans for future research in a UCLA news release,
“I believe that our research potentially points to a new treatment option. In the near future, I hope to initiate a phase 1/2 clinical trial for women with ovarian cancer tumors predicted to benefit from this combination therapy.”
In a first, researchers create inner ear tissue. From heart muscle to brain cells to insulin-producing cells, researchers have figured out how to make a long list of different human cell types using induced pluripotent stem cells (iPSCs) – cells taken from the body and reprogrammed into a stem cell-like state.
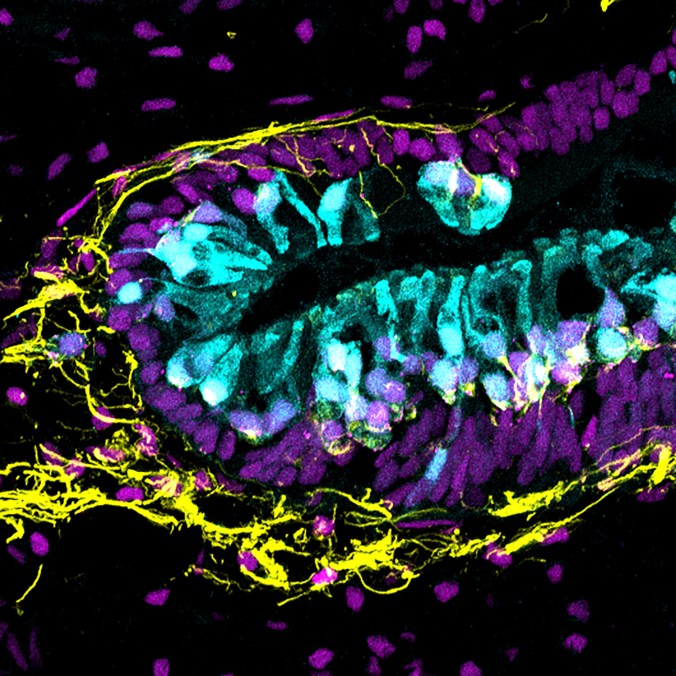
Human inner ear organoid with sensory hair cells (cyan) and sensory neurons (yellow). An antibody for the protein CTBP2 reveals cell nuclei as well as synapses between hair cells and neurons (magenta). | Photo: Karl Koehler
This week, a research group at the Indiana University School of Medicine successfully added inner ear cells to that list. This feat, published in Nature Biotechnology, is especially important given the fact that the inner ear is one of the few parts of the body that cannot be biopsied for further examination. With these cells in hands, new insights into the causes of hearing loss and balance disorders may be on the horizon.
The inner ear contains 75,000 sensory hair cells that convert sound waves into electrical signals to the brain. Loud noises, drug toxicity, and genetic mutations can permanently damage the hair cells leading to hearing loss and dizziness. Over 15% of the U.S. population have some form of hearing loss and that number swells to 67% for people over 75.
Due to the complex shape of the inner ear, the team grew the iPSCs into three dimensional balls of cells rather than growing them as a flat layer of cells on a petri dish. With educated guesses sprinkled in with some trial and error, the scientists, for the time, identified a recipe of proteins that stimulated the iPSCs to transform into inner ear tissue. And like any great recipe, it wasn’t so much the ingredient list but the timing that was key:
“If you apply these signals at the wrong time you can potentially generate a brain instead of an inner ear,” first author Dr. Karl Koehler said in an interview with Gizmodo. “The real breakthrough is that we figured out the exact timing to do each one of these [protein] treatments.”

Senior author, Eri Hashino, Ph.D., and first author, Karl R. Koehler, Ph.D. Photo: Indiana University
Careful examination shows that the tissue, referred to as organoids, not only contained the sensory hair cells of the inner ear cell but also nerve cells, or neurons, that are responsible for relaying the sound waves to the brain. Koehler explained the importance of this result in a press release:
“We also found neurons, like those that transmit signals from the ear to the brain, forming connections with sensory cells. This is an exciting feature of these organoids because both cell types are critical for proper hearing and balance.”
Though it’s still early days, these iPSC-derived inner ear organoids are a key step toward the ultimate goal of repairing hearing loss. Senior author, Dr. Eri Hashino, talked about the team’s approach to reach that goal:
“Up until now, potential drugs or therapies have been tested on animal cells, which often behave differently from human cells. We hope to discover new drugs capable of helping regenerate the sound-sending hair cells in the inner ear of those who have severe hearing problems.”
This man’s research is no fish tale
And finally, we leave you this week with a cool article and video by STAT. It features Dr. Leonard Zon of Harvard University and his many, many tanks full of zebrafish. This little fish has made a huge splash in understanding human development and disease. But don’t take my word for it, watch the video!